02. Current State: Austin State Hospital and Its Service Area

At an Integrated Service Design workshop led by the Design Institute for Health, Octavio Martinez, Tracy Asamoah, Amanda Flores, Sydney Harris, and Mike Geeslin review a presentation of the current state facility of ASH.
The first step toward redesigning the ASH Brain Health System was to define the current state of mental health care, starting with the ASH inpatient facility as a major focus, and then extending across the Service Area. To achieve this goal, we worked closely with HHSC, multiple regional stakeholders, and Meadows Mental Health Policy Institute (MMHPI) that provided significant data gathering and analytic services.
The Austin State Hospital
The Austin State Hospital was established as the State Lunatic Asylum in 1856 by an act of the 6th Texas Legislature and began caring for patients in 1861. It was renamed the Austin State Hospital in 1925. Austin State Hospital has a long history of caring for Texans struggling with mental illness. At times in its history, ASH was a cutting-edge provider of mental health care. However, following decades of deferred maintenance, the poor quality of the buildings makes delivering modern care difficult and only possible through heroic efforts of a committed staff. The Cannon Report in 2014 determined that 49% of the buildings on the ASH campus were in “poor” or “critical” condition, and they have not improved since. Consequently, renovation is simply not an option and replacement is necessary.
ASH Capacity
Austin State Hospital has physical capacity for up to 299 inpatient beds and an operational budget for up to 263 beds; for FY18 it operated at 252 beds. These beds are often provided with multiple individuals to a room (as many as four), contrary to current clinical recommendations of one person per room. The beds can be categorized as described in Table 2. In the past few years, pressure for more adult beds, particularly for ‘forensic’ patients, has necessitated shifting Specialty Unit capacity to accommodate this need.
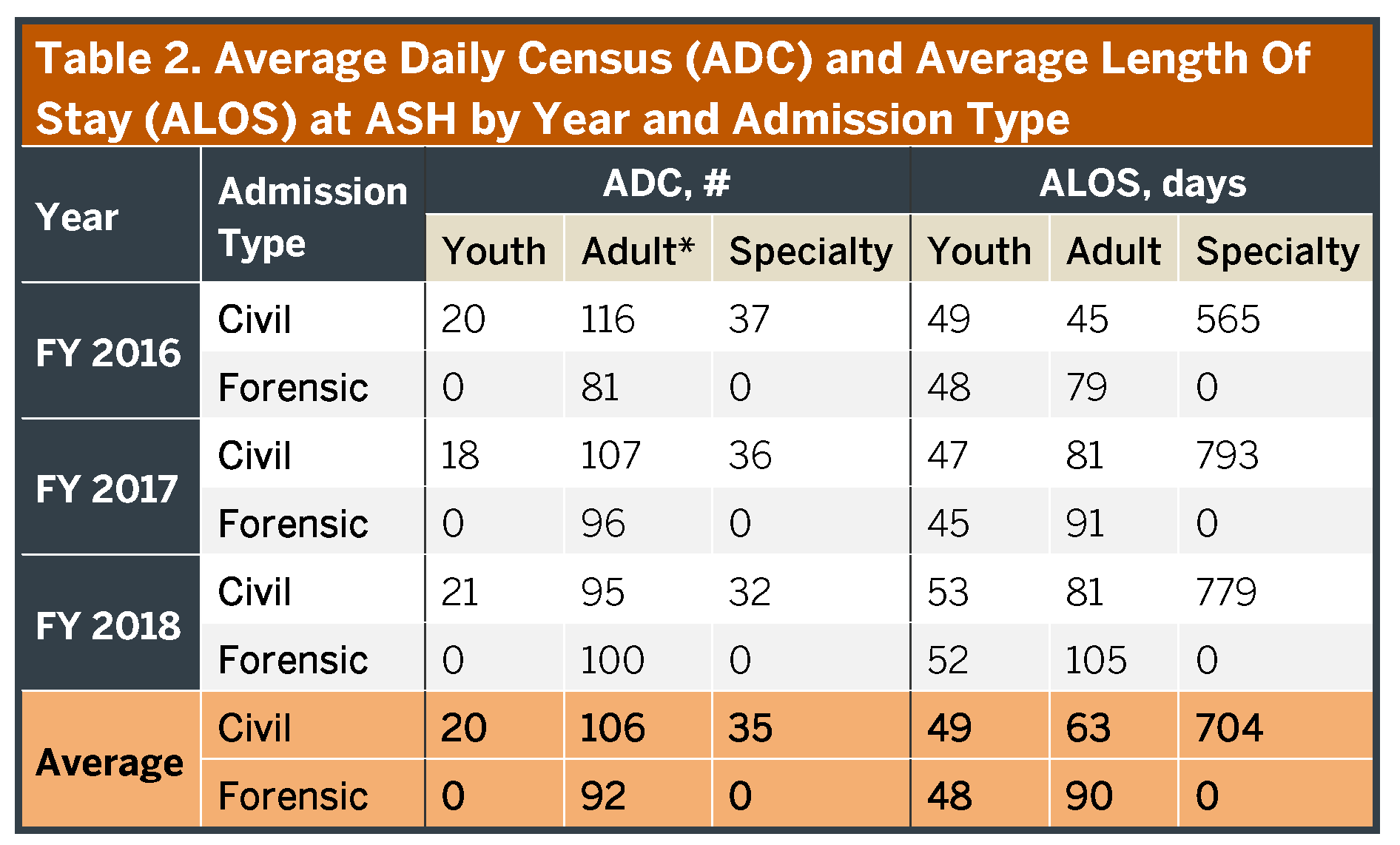
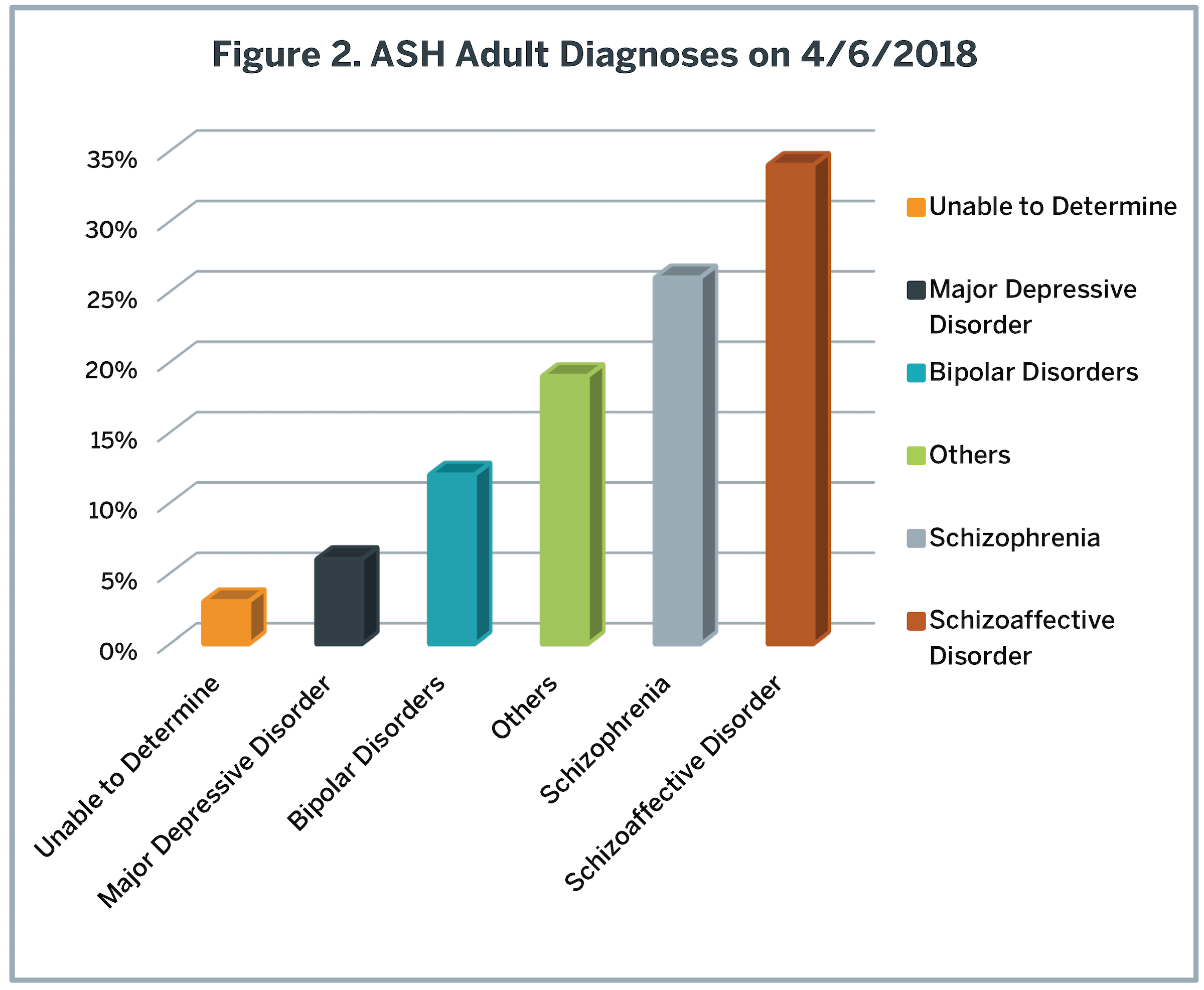
Austin State Hospital provides care for patients of all ages, although primarily it serves young and middle-aged adults with severe and persistent mental illnesses such as schizophrenia or bipolar disorder (Figure 2). Individuals needing care are typically referred to ASH from jails (by criminal court order), LMHAs, emergency departments, probate courts and other hospitals; the latter are people whose current episode of care cannot be completed with the short-term stabilization approach typical of most private psychiatric facilities. Consequently, in addition to other functions, ASH serves as a safety net for treatment unresponsive individuals. Austin State Hospital only rarely provides direct admissions (i.e., walk-ins), and it is not well designed for that function. It operates at full capacity essentially all of the time. Although inpatient capacity is often interpreted simply as the number of available patient beds, in fact it is heavily dependent on the rate beds can be turned, i.e., how long a specific individual stays in the hospital before the bed can be re-used. Table 2 provides the average length of stay (ALOS) for people in each of the key subcategories. In the past 6 years, the ALOS for an individual discharged from ASH has increased from around 30 days to those listed in Table 2. This change reflects both an increasing number of ‘forensic’ individuals with legal charges (who stay longer) and a dramatic increase in how long ‘civil’ (without legal charges) patients are staying (see Appendix 8 for details). Based on these ALOS, beds in ASH turn only 3.7 times/year. Consequently, discharging patients less than every four months, on average, decreases capacity for new admissions and access to care. In part, this slow turn rate reflects a significant number of individuals (approximately 70) who effectively reside long-term at Austin State Hospital. If the long-stay individuals are excluded, the bed turn rate is faster, but still infrequent (4.7 turns/year) and involves fewer available beds. This slow turn rate has created forensic and civil waitlists of 75 and 20 people/day respectively. Approximately two-thirds of the forensic waitlist is in Travis County, and no more than six people on any other waitlist throughout the Service Area.
The Cannon Report in 2014 determined that 49% of the buildings on the ASH campus were in ‘poor’ or ‘critical’ condition…
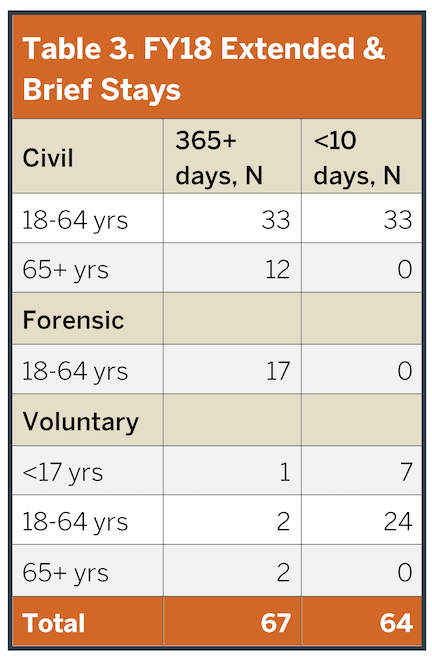
The number of individuals experiencing extended (>365 days) and brief (<10 days) stays are illustrated in Table 3. These data highlight several key aspects of ASH function. First, ASH is rarely used as a short-term, acute stabilization hospital. Less than 10% of ASH discharges in recent years occurred after hospital stays of less than 10 days. Second, due to a myriad of barriers to discharge, as noted a significant number of ASH beds function as residential care, in which individuals essentially live at the hospital irrespective of clinical need. At this time, this latter function includes nearly 70 people, effectively taking those beds off-line for new admissions. These individuals have an ALOS approaching 3 years (and growing). Therefore, the true capacity for new admissions is reduced to only approximately 155 adult beds. Finally, ASH is substantially serving forensic patients, i.e. individuals with legal charges needing competency restoration to stand trial. Competency restoration is a legal term referring to the ability of a person to understand and participate in criminal court proceedings; it may or may not correlate with the individual’s clinical needs. Details about competency restoration and recommendations to change these processes are provided later in this report.
…essentially [70 people] live at the hospital irrespective of clinical need… effectively taking those beds off-line for new admissions.
The increasing pressure on capacity for competency restoration suggests at times that ASH functions as an extension of the legal system rather than as a health care provider. The percentage of patients with legal charges at ASH has increased from 41% in FY16 to 51% in FY18, and it continues to rise. This increase is not unique to ASH, but is true across all of the state’s public inpatient facilities. Currently, the legal system dictates when individuals with legal charges can be discharged, so that they often remain hospitalized longer than deemed clinically necessary by ASH staff. For example, in a recent analysis, the ASH leadership determined that 41% of the forensic bed days occurred after individuals were either determined competent to stand trial or not likely to regain competency (Appendix 8). In general, competency restoration can be completed within 60 days and typically in less than 3 weeks (Austin State Hospital, 2018), which is inconsistent with the current ‘forensic’ length of stay of 92 days. Illustrating this point, in the first quarter of 2018, individuals remaining in ASH after needing additional competency restoration contributed 4,039 days of hospitalization; these days could have alternatively accommodated over 60 additional people needing care in that interval (based upon a 60-day length of stay). Unfortunately, some individuals stay in the hospital longer than they would in jail under conviction for their charge, even though there is clear evidence that competency can be safely restored in the community (Mikolajewski et al., 2017).
In addition to these general adult beds, ASH operates a 30-bed child and adolescent psychiatric services (CAPS) with an average daily census of 20 individuals. These youth rarely have accompanying legal charges and stay in the hospital for shorter periods than adults (Table 2). Unlike adults, ASH does not report a significant regional waitlist for admission into this unit, as most children and adolescents are treated in private psychiatric facilities through Community Psychiatric Bed (CPB) funding with the LMHAs or insurance, including Medicaid or CHIP. The CAPS unit is located separately from the main ASH campus (across 45th street) and the building has been rated as FCI=0.24 (fair condition). The typical patients are 10-year-old children and 16-year-old adolescents with diagnoses of mood, adjustment and/or cognitive disorders. However, these youth are often dually diagnosed with a mental illness plus, e.g., substance use disorder or intellectual developmental disabilities (IDD). Generally, these young individuals are eligible for Texas Medicaid, so private placements closer to the child’s home are a better option when available. Nonetheless, some of these youth need longer treatment than Medicaid will pay for at a private facility, leading to an ASH referral. Residential Treatment Centers (RTC), including the Waco Center for Youth and several private facilities in the Service Area, also contribute to inpatient care for adolescents. Additional details re: CAPS in the region are provided in Appendix 9.
…competency restoration can be completed within 60 days and typically in less than 3 weeks.
The campus also operates a Specialty Adult unit with a capacity of 72 beds although many of these beds have been shifted to manage general adults as noted previously. These individuals have significantly longer lengths of stay than do the other units (Table 2), related to barriers to placement into less restrictive settings. In contrast to the general adult units, there is no waitlist for admissions to the Specialty Unit. Additionally, only rarely do these individuals have ongoing legal charges. Although a mix of individuals occupy this unit, the typical person has an average age of 47 years with diagnoses of schizoaffective disorder, schizophrenia or bipolar disorder and often a comorbid diagnosis of, e.g., IDD. Many of these individuals are eligible for Texas Medicaid or Medicare so could be better served in other private or public facilities, particularly those specializing in long-term residential care, if barriers to discharge could be eliminated.
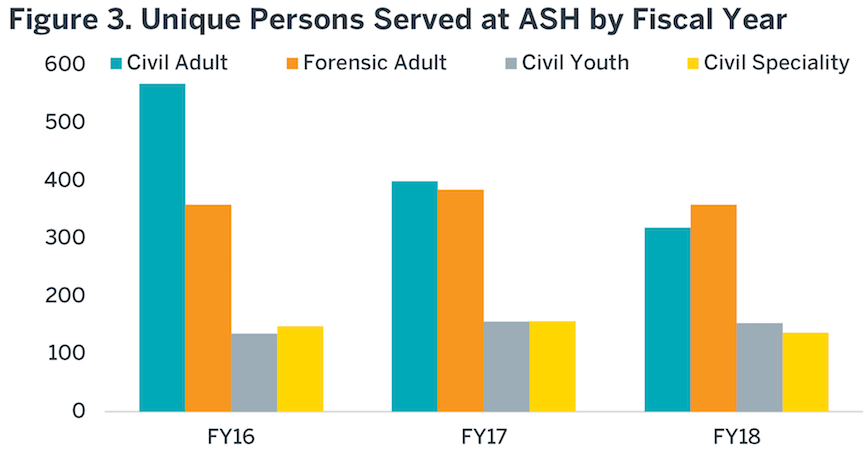
During the last several years, the total number of individuals treated annually at ASH has steadily declined, due to increasing lengths of stay for admitted individuals. The trend of these data are illustrated in Figure 3. During FY18, ASH treated approximately 1000 unique individuals. If lengths of stay continue to increase, this number will continue to decline.
ASH Operations
The State Hospital System within HHSC manages all of the state hospitals including Austin State Hospital. Health and Human Services Commission employs approximately 60,000 people, of which ASH employees represent less than 2%. Although only a small fraction of HHSC, the work performed by ASH is impactful and must be effective and efficient to support the needs of the 75 counties it serves.
…as many as four people might occupy a single small room.
As stated earlier, a committed staff provides the best quality of care possible to those served within Austin State Hospital. From qualitative research completed through observations of an adult psychiatric unit in ASH and several interviews with ASH providers, the deteriorating building impairs operation (Appendix 10). Within the adult psychiatric units, our team found limited private space for people receiving care to engage with their providers; this challenge left staff and patients feeling as though they were being watched all the time, and certainly challenges privacy rules with care delivery. Despite being large buildings on a large campus, the outmoded design limits functional space and places for individuals’ who are stressed or agitated to retreat (as noted previously, as many as four people might occupy a single small room). These experiences negatively impact patient engagement and satisfaction even when good quality care is provided. Limited areas to retreat increase the risk of violence for patients and staff.
HHSC reports quarterly on their nine hospitals’ performance within the State Hospital System 2018 Management plan (Appendix 11). This document contains measures of financial indicators, clinical quality, and access. Datasets are reported to the LBB to indicate how well each hospital is operating; however, the report is 202 pages long with so many metrics that it is unclear how hospital leadership is expected to focus on continuous quality improvement in any specific area. This large number of metrics with limited prioritization is the opposite approach to how better health care systems manage continuous quality improvement. One of the metrics measured is the Mental Health Statistics Improvement Project (MHSIP) NRI Inpatient Consumer Survey to gather patient satisfaction ratings. Health Human Services Commission set a goal to receive 25% participation across all state hospitals. This goal is very conservative, particularly for individuals receiving care for the extended duration of a state hospital, and yet is achieved at ASH only 18% of the time, placing it among the two lowest of all of the Texas State Hospitals (Appendix 11, p. 60). When individuals do complete the survey, they provide an average score of 3.45 out of 5 on the MHSIP NRI Inpatient Consumer Survey, again the second lowest among the state hospitals (Appendix 11, p. 61). Although ASH historically also failed to meet the annual patient grievance score of less than 3/1,000 bed days, during the last 2 years, ASH staff have significantly improved this rating, so is now performing at or better than the benchmark (Appendix 11, p. 65).
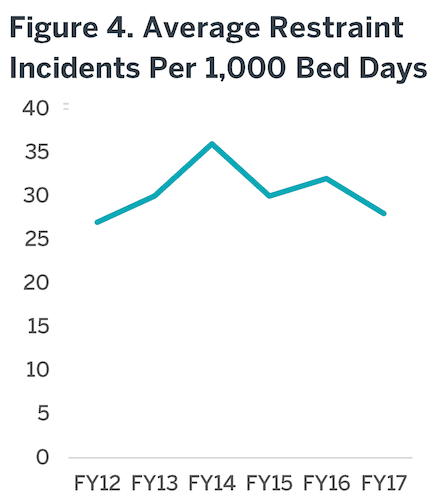
Two important clinical quality measures in psychiatric facilities are the rates of restraint and seclusion. The American Psychiatric Nurses Association (APNA) set a goal for all restraints and seclusion to be eliminated. The use of these practices are traumatic to the person receiving services and to the staff applying the restraints. Nationally, restraints and seclusions have been linked to as many as 150 deaths annually as well as staff injury, time off and turnover (SAMHSA). Over the last few years, ASH has had the second highest rate of use of restraints among Texas State Hospitals (31.1/1,000 bed days), although this rate is improving during the past year (Figure 4). Seclusion is used relatively infrequently at ASH, in part due to limitations of the physical plant.
The Center for Medicare and Medicaid (CMS), publishes the Inpatient Psychiatric Facility Quality Reporting Program that shares rates on restraints for 1653 psychiatric facilities (CMSReport). In 2016, ASH reported their annual hours of restraint use per 1000 patient beds as 0.63 hours. In comparison to other hospitals, 83% were less than .49 hours and 26% had 0 hours in restraints.
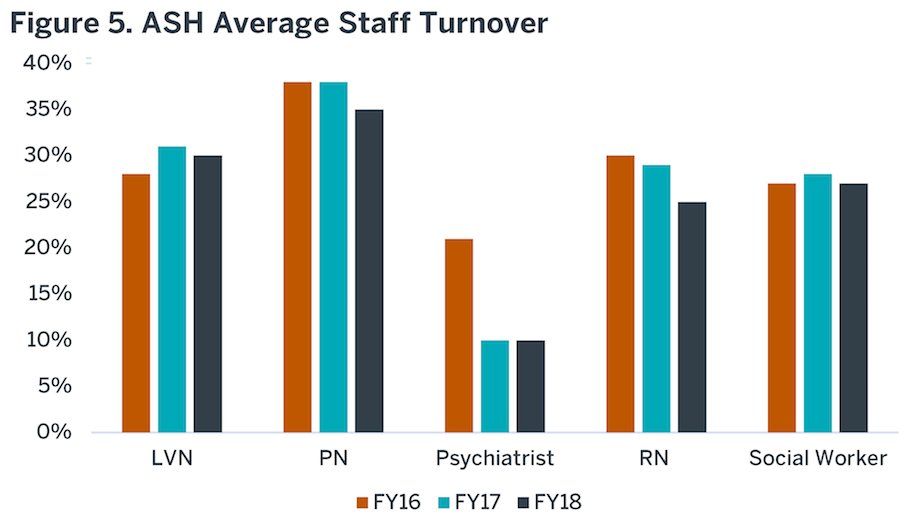
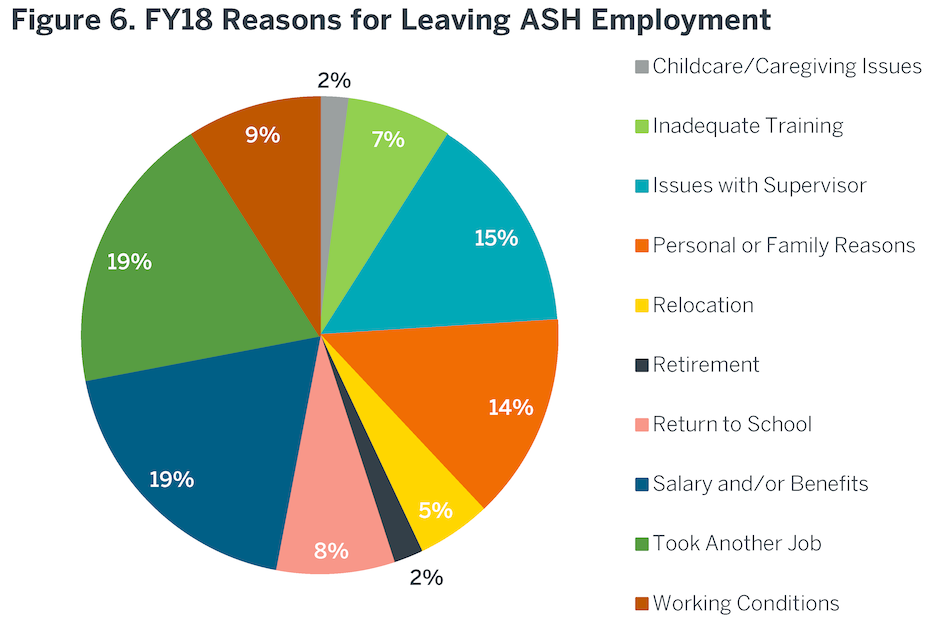
The quarterly report does not provide an employee satisfaction rating. Employee satisfaction is strongly linked to patient satisfaction. However, there is a high turnover rate for staff. Figure 5 illustrates the annual turnover rate for staff of FY17 – FY18Q2. High staff turnover negatively influences morale, operations and team esprit de corp. Outside the Operational Plan, HHSC does collect satisfaction ratings from staff at their exit interviews (Figure 6). The most common reasons included issues with supervisors, dissatisfaction with salary/benefits and better opportunities. As discussed in the Workforce section of this report, ASH salaries are lower than the Austin community standard.
ASH Costs
Health and Human Services Commission reports the daily cost of a bed at ASH as $567; in comparison, an average private bed daily cost approaches $1,000. However, in the HHSC calculation, not all benefits or the central infrastructure expenses are loaded into this cost estimate, as they are with private hospital bed calculations. When full central and benefits costs are included (as per the industry norm), the actual per diem bed cost is $752. When contracting with community hospitals across the state, the average purchased Community Psychiatric Bed (CPB) negotiated rate (i.e., what the government pays) averages $627; this rate averages $703 in the ASH Service Area. Medicaid pays $529. These variable rates reflect the typical disconnects between true costs and payment structures in health care in general that confound planning for expenses of inpatient psychiatric care. The higher fully-loaded costs in a private facility reflect the rapid stabilization function they provide. Specifically, the work flow in a private, short-term hospital in which the goal is acute stabilization and rapid discharge back into ambulatory care (usually with admissions lasting less than 10 days), requires daily physician rounds, admissions and discharges 7 days/week, with immediate attention to discharge planning upon admission, and close collaboration with ambulatory resources. Austin State Hospital is not designed by either staffing or workflow for short-term acute stabilization. For example, treatment teams round with the physician less than weekly, discharge planning can be delayed, especially in forensic cases, and the hospital is not equipped for weekend or evening discharges. Regardless, after negotiations, the per diem cost at ASH is similar to that of a private facility.
…residing for a year at ASH costs approximately $275,000 whereas in a residential care facility the same person’s care would cost approximately $55,000.
The daily cost at ASH exceeds that of a typical longer-stay residential care facility (approximately $150/day), even though nearly one-quarter of ASH beds are used in this manner. This observation means that the annual cost of care is much higher in ASH than it might be in a more appropriate setting for these individuals. For example, an individual residing for a year at ASH costs approximately $275,000 whereas in a residential care facility the same person’s care would cost approximately $55,000. Moreover, the latter would provide more appropriate care as it would be designed for the specific residential need. The ASH workflow and cost structure suggests that it is optimally designed for medium-term (e.g., up to 60 days) subacute care. Several factors contribute to bed-day costs being relatively high based upon existing ASH services: 1) the hospital is performing functions for which it is not optimally designed either structurally or by workflow; 2) additional staffing and overhead are needed to provide good clinical care in a facility long-past its ability to support such care; 3) the burdensome risk-aversive requirements of a state bureaucracy adds inefficiencies and embedded costs; and 4) the needs of increasing numbers of forensic patients adds costs compared to civil patient care.
As noted, there are overhead costs buried in the large HHSC bureaucracy that are consequently difficult to identify and manage. These diverse factors hamper developing efficient and effective clinical workflows to advance new patient care models. With the new building designed for the care ASH is actually providing, HHSC will be better positioned to optimize workflow and staffing to manage costs within its current complex bureaucratic structure.
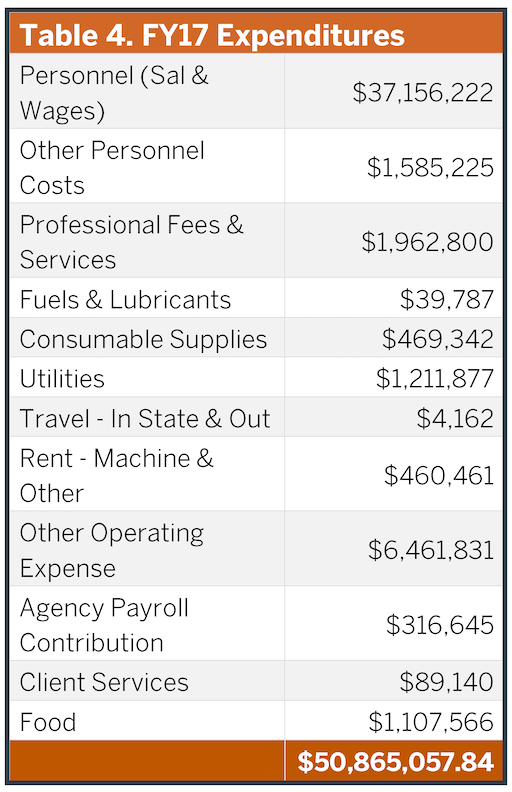
In the last several fiscal years, ASH’s total annual operating budget has been $51M (Table 4) with approximately $5M in annual patient collections (e.g., Medicare, Medicaid). There is another $18M in benefits and HHSC central allocations. Most expenditures are in personnel ($37M), and the listed costs do not include benefits as they are managed separately in HHSC (although still exist). Current staffing includes 22 Psychiatrists, 12 Psychologists, 130 Nurses, 29 Social Workers, 334 Psychiatric Nurse Assistants, 10 Security Officers and 368 other staff. Based upon the current bed-day costs previously discussed, this budget can support approximately 263 operational beds per year. This limitation ultimately places a cap on the size of a new facility in the absence of additional operational funding, greater operational efficiencies, or redesign of the service system in which ASH resides. These considerations are discussed in more detail later in this report.
Key Points – ASH Current State
• The Austin State Hospital must be replaced.• In FY18 ASH operated at 252 beds including 30 beds for youth. It is always at full capacity.
• The structure and workflow of the hospital better supports long-term subacute care than acute stabilization or residential care.
• Approximately 70 individuals essentially live at the hospital, taking those beds “off-line.”
• The average ASH bed turns over less than 4 times per year.
• ASH increasingly serves individuals with legal charges admitted for competency restoration; their average length of stay exceeds what is expected for this function.
• The daily cost of a bed at ASH is higher than a number of alternative treatment options that are likely more appropriate for many of the individuals currently being treated there.
• The complex HHSC infrastructure impacts ASH management and performance.
• Approximately 95 people each day are waiting in jails or elsewhere for a bed at ASH.
