02. Overview And Background
Phase I ASH Redesign
Texas aims to be a national leader in mental health care and so to that end made substantial investments during the past decade. Significant progress began when the Cannon Report (2014) identified that most of Texas’ adult public psychiatric hospitals were in “poor” and “critical” condition, and five needed to be razed and replaced, which included the Austin State Hospital (ASH). The Cannon Report (Appendix 1) and HHSC’s A Comprehensive Plan for State-Funded Inpatient Mental Health Services (Appendix 2) established the basis for replacing the current ASH. The 85th Texas Legislature invested $300M to create construction planning of the outdated public psychiatric hospital system. The legislature encouraged partnerships with academia to complete the construction planning. This encouragement and investment led to a partnership between the University of Texas at Austin’s Dell Medical School (Dell Med) and Texas Health and Human Services Commission (HHSC) to develop the plan for a new ASH facility and a continuum of care for the regions served by ASH.
The initial investment ($15.5M) from the 85th Texas Legislature established Phase I of the ASH Redesign, namely to develop a Master Plan (Appendix 3) and a blueprint of the ASH service area continuum of care (Appendix 4). The full report can be found at ashredesign.org. Phase I established a Steering Committee to lead the efforts of the ASH Redesign, which then created a first round of subcommittees (116 members) to gain insight and strategies toward an efficient system for a new ASH. Through qualitative research, the team learned that the term “brain health” was less stigmatizing than “mental health” by clarifying that these conditions impact brain function and have a physiological component. However, the term “mental health” is more commonly used and understood. Throughout the report, then, we will interchangeably use both terms as a step toward decreasing stigma.
…we will interchangeably use both terms, “brain health” and “mental health”, as a step toward decreasing stigma.
World Class Hospital

Phase I included designing a new world class hospital for Texans on the ASH campus. Following the procurement processes of the University of Texas, Page Southerland Page, Inc. (Page/) was subcontracted to complete the hospital design in partnership with architecture+; the latter are experts in the design and planning of advanced psychiatric facilities.
The new ASH design will enhance healing and recovery for people by improving the physical space to allow modern evidence-based care. The new hospital will be comprised of ten 24-bed living units, each with three 8-bed sub-clusters, totaling 240 beds. The living units constitute a “neighborhood” that includes a large dining hall, porches, activity and quiet rooms, and an open care desk. People receiving care will have their own bedroom and bathroom, providing privacy and space to recover. The building takes advantage of the slope of the land, allowing the hospital to be two- and three-stories at different parts of the site, which is a more cost-effective use of space than the current 1-story design. The new hospital provides access to eleven court yards. Most units will be only one flight of stairs from courtyard access; outdoor access is known to facilitate recovery. People receiving care will progress through the hospital in a way that mirrors the recovery process. A person will experience their individual space, the neighborhood of their living unit, a treatment mall and finally the downtown gathering space. All of these steps will help them return to their community to continue recovery.
The new ASH design will enhance healing and recovery for people by improving the physical space to allow modern evidence-based care.
Phase II ASH Redesign
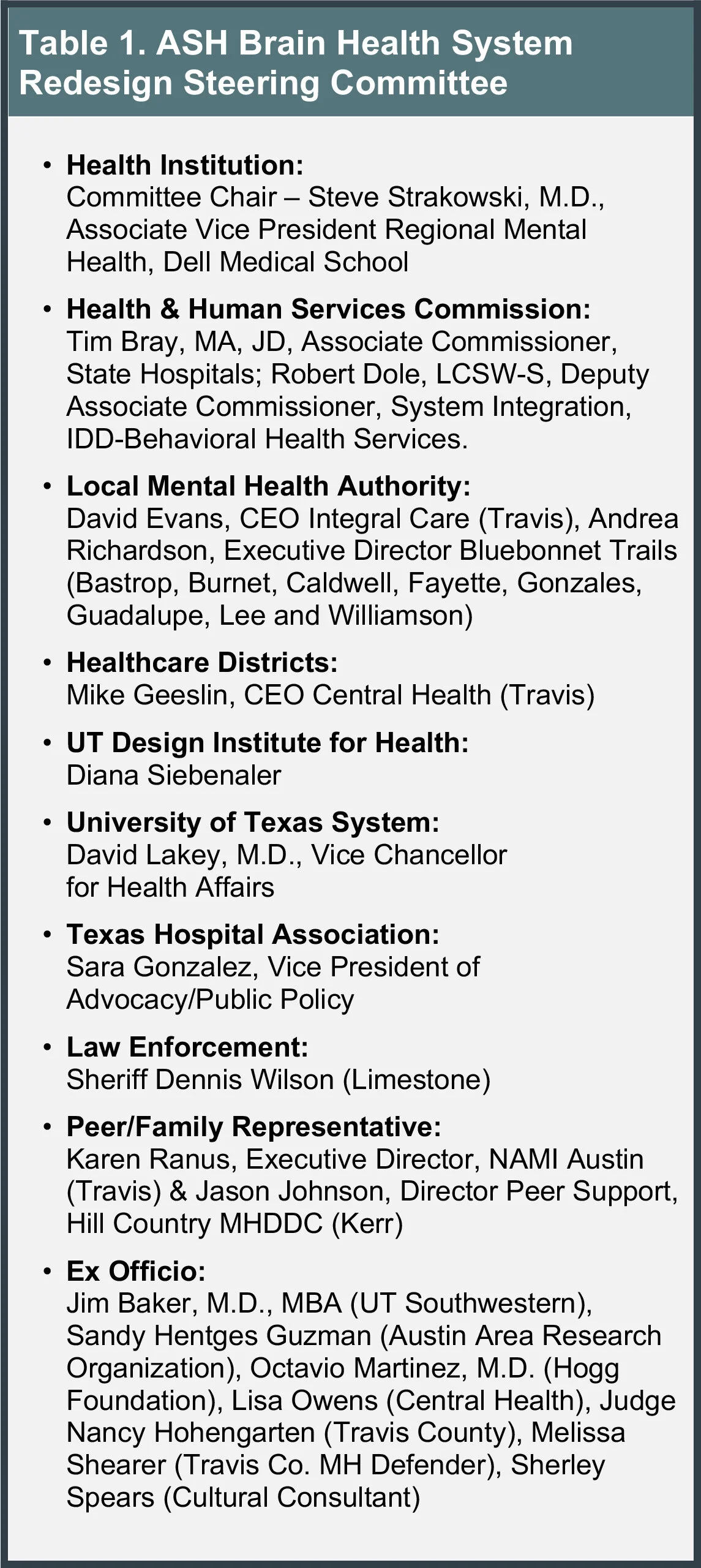
In the 86th Legislative Session, over $445M was approved to improve the state hospital system. HHSC was appropriated $165M to begin construction of the new ASH and continue the ASH Redesign. After completion of Phase I, the Steering Committee continued to meet and support the planning and design efforts for the new ASH. Since our initial report, many of the same stakeholders remain engaged in the ASH Redesign efforts, detailed in Table 1 and the Steering Committee Charter (Appendix 5). Following procurement processes of the University of Texas, Turner Construction Company (TCCO) was subcontracted as the construction manager at risk to build the new hospital.
The Steering Committee created work groups linked to previous report recommendations. A total of 69 members volunteered their expertise and time in six work groups:
Competency Restoration
Hospital Clinical Strategies
Campus & Continuum Clinical Strategies
Campus Planning Partnerships
Peer & Family
History of ASH
Charters were developed for each work group to establish guidelines and goals to coordinate efforts to develop the recommendations provided in this report (Appendix 6):
Key Points – ASH Redesign Phases:
• Texas lawmakers invested over $745M in mental health.
• ASH Redesign Phases I and II establish recommendations to create
an efficient system to support the new ASH.
• Page/ with architecture+ designed and Turner Construction Co. is
building the new ASH.
ASH Service Area
Texas state hospitals accept referrals from any region in Texas; however, each hospital primarily serves a designated area. The ASH service area extends from the eastern border of Newton County to the southwestern boarder of Val Verde County, covering 75 counties. The 75 counties are separated by age group as illustrated in Figure 1.
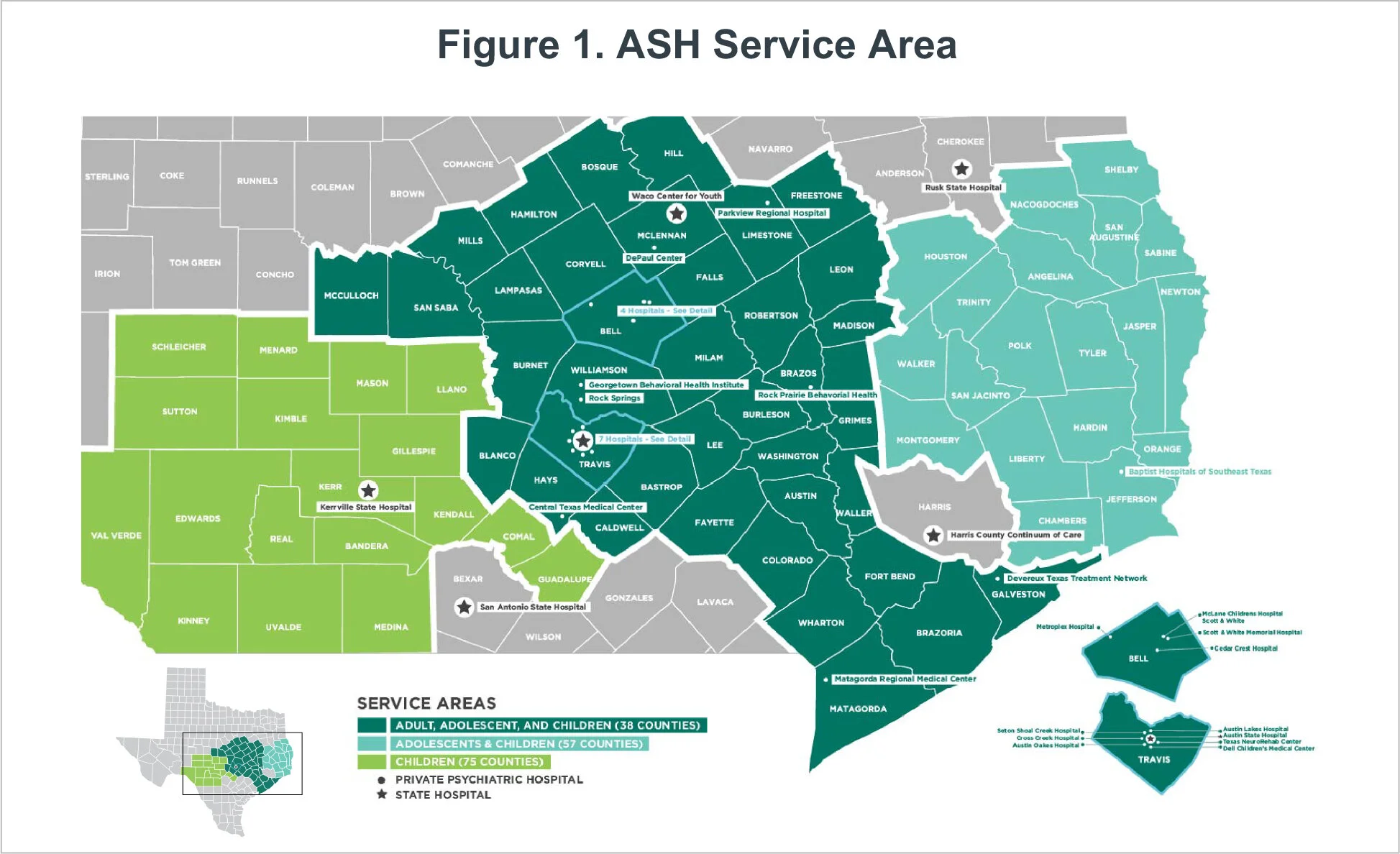
Specifically, 38 counties refer adults, adolescents and children needing hospital care, 19 refer adolescents and children (not adults), and 18 refer only children. ASH is located in Central Austin on approximately 95 acres. Under typical circumstances, ASH has ~263 available beds divided among four hospital buildings. On the main campus, care for adults is provided in two hospital buildings (152 total beds), care for elderly and intellectual disabilities is provided in one building (83 total beds) and children and adolescent care is provided in a fourth building across 45th street (28 total beds). The hospital’s response to the global health pandemic has required many of these beds to be managed differently while we wait for the crisis to resolve.
The Master Plan (Appendix 3) established key goals, calculated capacity and determined a biennial budget for a new facility. Two factors that played into the final physical capacity of the new adult ASH were:
ASH’s budget has remained flat for several years, and routinely operates within a budget ($50M annually) that can maximally operate only 265 beds for adults and children. Consequently, the redesign could not increase the capacity in the absence of assurances of more operating funds; and
The redesign team worked with other sites in Texas where hospital expansions and construction were occurring as part of a statewide strategy to diminish the waitlists.
Our first ASH Redesign report presented three different facility options for the ASH Campus: A) 240-bed adult hospital costing $283M, B) 216 – 240 bed adult hospital with 48 – 70 bed residential facility costing $288-330M, and C) 264 – 288 adult bed hospital costing $311-330M. Based on the two guidelines listed, option A was selected to move forward.
Phase I of the ASH Redesign also reviewed the children and adolescent hospital; however, the building was found to be in fair condition and rarely has a waitlist for admittance. HHSC has continued to maintain the building to provide quality care. Consequently, no new construction was recommended for the children’s hospital building at this time while we identify alternative solutions to providing better child psychiatric care (e.g., as provided by the statewide networks created by SB11 in the 86th legislative session).
ASH Admissions
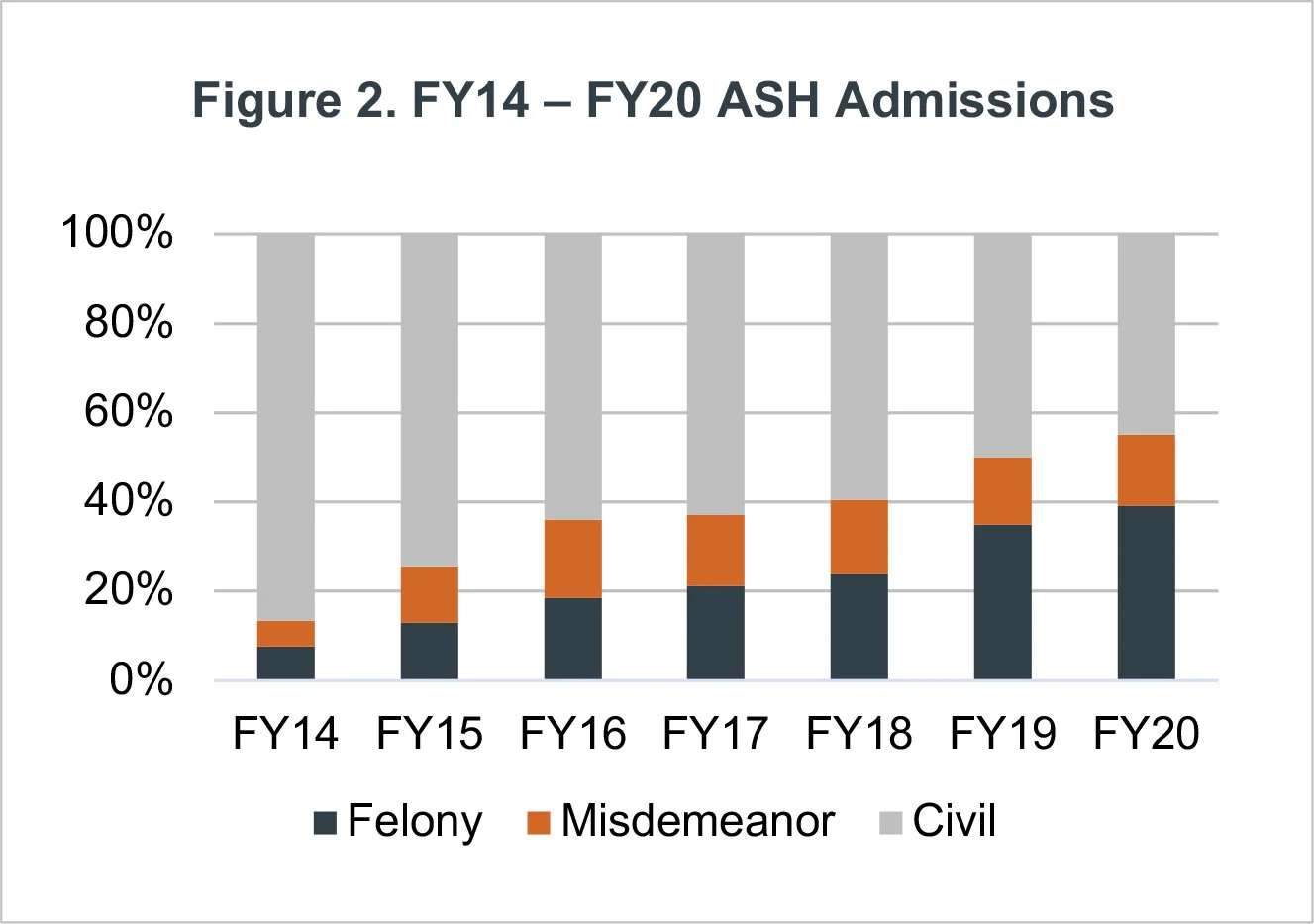
ASH treats approximately 900 people annually. Most individuals admitted to ASH are on a forensic commitment; i.e., the process used to raise a person’s ability to participate in his or her own legal defense through inpatient competency restoration (further details are found in the section Forensic Roadmap Strategy). Figure 2 illustrates the growing percentage of people at ASH on a forensic commitment, with a corresponding decreasing percentage of civil admissions. Civil commitment is a process in which people unable to care for themselves or who are an imminent risk to themselves or others, are involuntarily referred for inpatient psychiatric care. Both civil and forensic commitments deserve care in the least restrictive setting based upon their level of care needed. The increase in forensic bed use and decrease of civil bed use at ASH reflects statewide and national trends, so is not unique. The National Association of State Mental Health Program Directors reported a 76% increase of forensic referrals in state hospitals from 1999 – 2014 (2017). Subsequently within this report, we propose strategies to assist in the efficiency of how the new ASH might support the forensic pathway and develop tactics to improve processes at the intersection of legal and mental health systems.
ASH treats approximately 900 people annually.
The ASH service area includes a total of twelve local mental health authorities (LMHAs), nine of which support the core 38 counties. Based on CY 2019 estimates from the US Census Bureau, ASH and LMHAs in the adult counties supported a population of 4,180,000 people, a twelve percent increase from 2018. When people experience a crisis leading to the emergency room or jail, LMHAs are one community resource responsible for referring people needing hospital-level care to ASH. LMHAs are key components of mental health care in the ASH service area; they provide critical services to ensure people remain in their communities for care as much as possible to continue their recovery. Nearly always, individuals referred to ASH experience a delay before admittance.
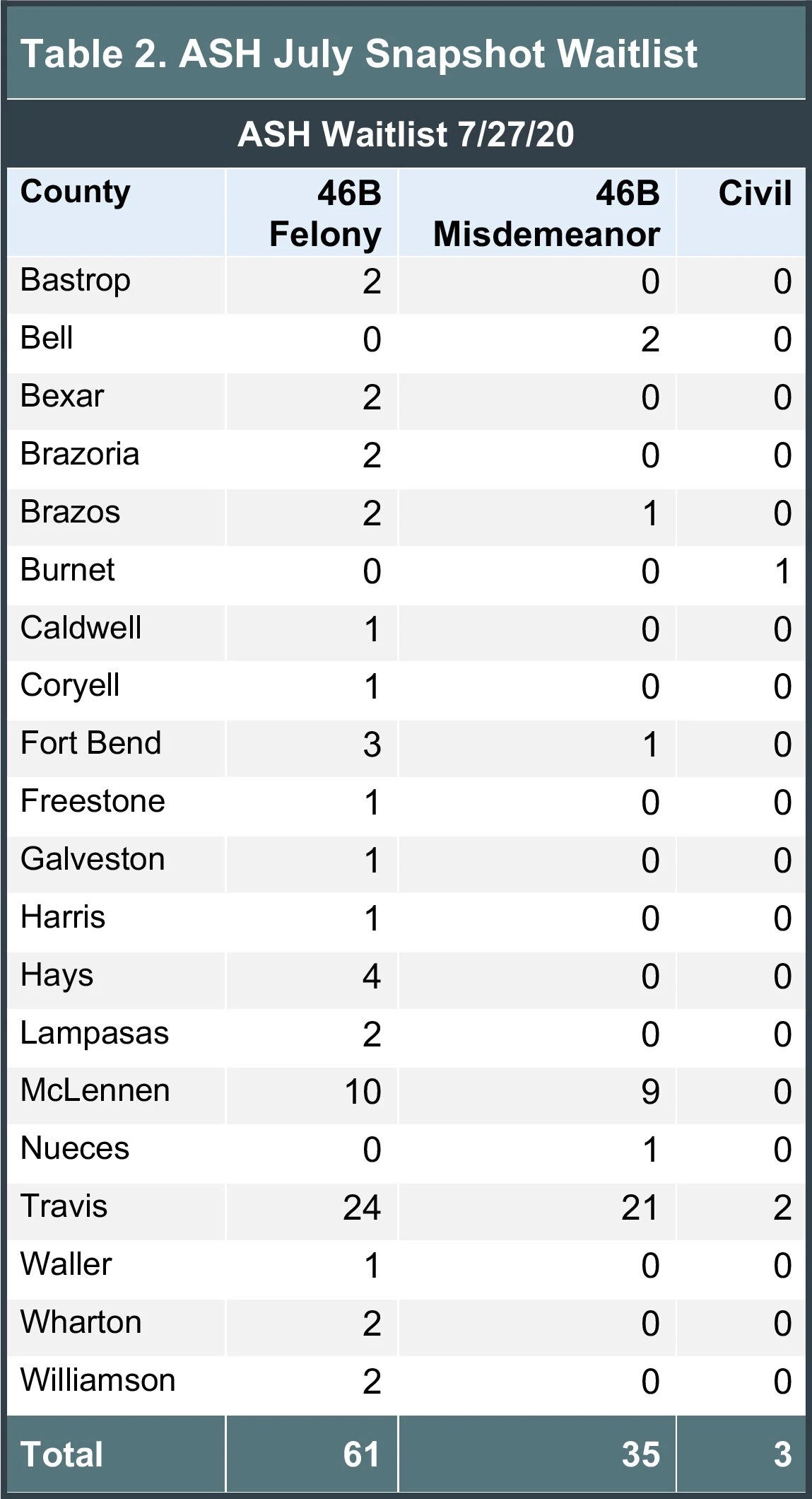
ASH is always full, so when a bed becomes available it is provided to a person on the waitlist. As of the time of this publication, there are more than 1,000 people waiting for a state psychiatric bed in Texas, and about 95 people are waiting for a bed at ASH specifically. Most people on the waitlist are waiting in jail or in an emergency room. Table 2 is a snapshot of ASH’s waitlist in July 2020; as can be seen, Travis County (47) had the most people waiting, followed by McLennan County (19).
This waitlist is managed by HHSC, tracking available beds for the state and then notifying emergency departments, law enforcement, or LMHAs when a bed becomes available. Although a service area is designated to provide care somewhat closer to a person’s community, as noted previously, some people receive care from a state hospital outside of their service area if a bed is available more readily than one locally. From FY15 – FY20, out of district counties use 13% of ASH bed days.
As of the time of this publication, there are more than 1,000 people waiting for a state psychiatric bed in Texas, and about 95 people are waiting for a bed at ASH specifically.
The state hospital system is the most intensive level of public mental health care available to Texans. The ASH Redesign is one of five current State Hospital construction projects. The other four projects include: 1) Rusk State Hospital, which is converting 60 existing beds to maximum-security beds (MSU); 2) Kerrville State Hospital, which is adding 70 new MSU beds; 3) UTHealth in Houston, which is adding a new hospital tower (UT Health Behavioral Sciences Center) of up to 264 short-term beds adjacent to Houston’s Harris County Psychiatric Center; and 4) San Antonio State Hospital, which is replacing the current hospital and separately adding 40 new beds. These additional beds, especially the new hospital in Houston, provide an opportunity to realign service areas to care for more people closer to their home communities. For example, a person from Galveston or Brazoria Counties needing inpatient care might currently bypass the facility in Houston to be brought to Austin. In the future, they would receive care in the new hospital in Houston rather than come to ASH. The unnecessary extended drive is cumbersome, inefficient and costly, as well as suboptimal care for a vulnerable person.
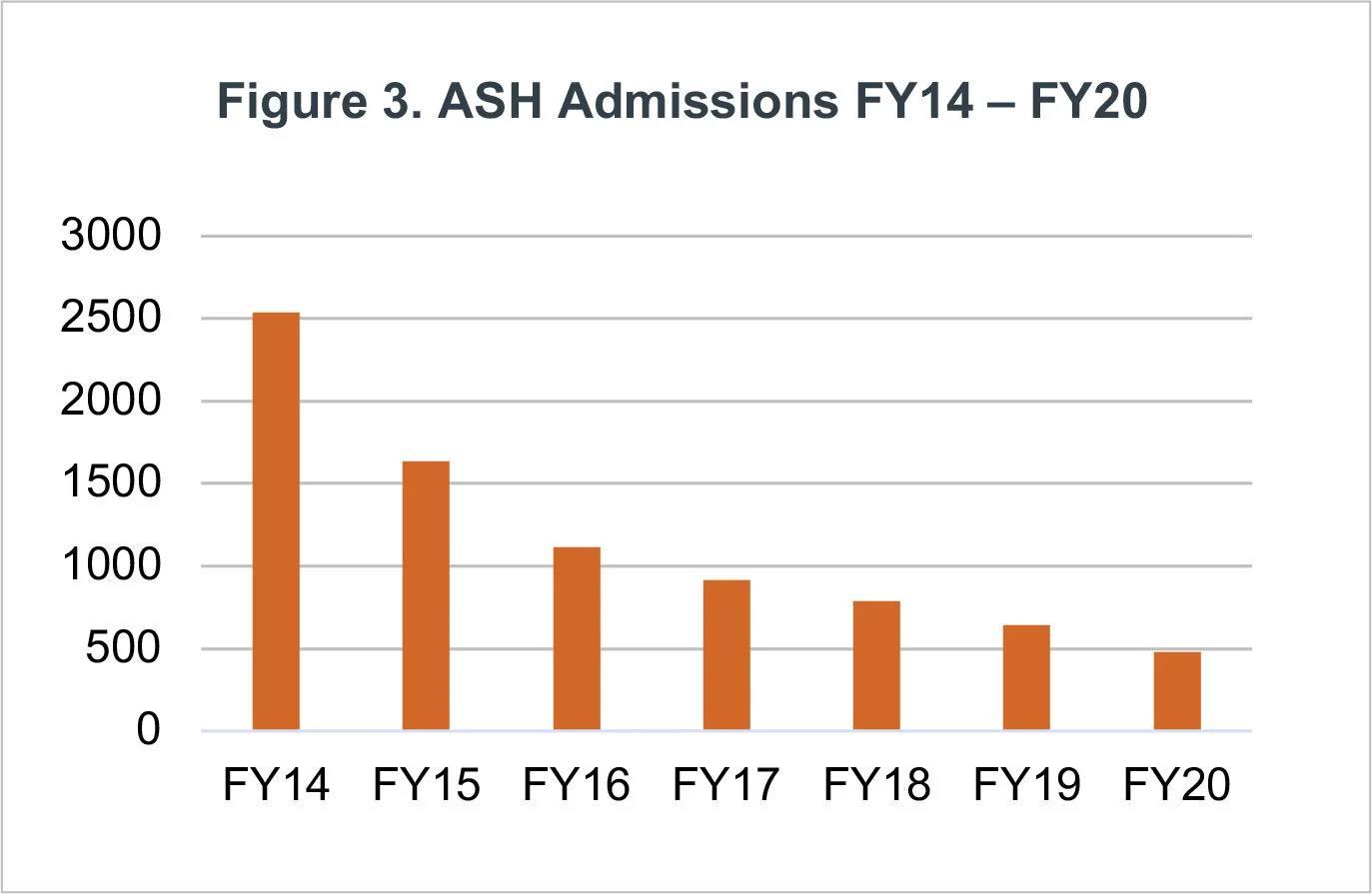
Notably, admission rates to ASH have decreased throughout the last several years. Figure 3 presents the change in new admissions from FY14 through FY20. Several factors contribute to this trend. The average length of stay for adults is increasing for both civil and forensic populations. Specific to the forensic population, many of the patients are experiencing extended commitments, requiring them to stay beyond their initial 60-day commitment to, at times, greater than 120 days (details in Forensic Roadmap Strategy). For the civil population, the acuity level of admissions exceeds what may be available by local psychiatric hospitals and crisis units, resulting in extended lengths of stay at ASH. Additionally, persistent barriers to discharge from ASH contribute to the hospital continually operating at capacity. Together, these factors combine to decrease the functional capacity of ASH (and each of the state hospitals).
Barriers to Discharge
ASH identifies and monitors individuals who have been in the hospital for more than 365 days to define reasons they are unable to successfully discharge from the facility. At the date of this writing, over 60 people experience a barrier to discharge from the hospital into a more appropriate, less restrictive level of care. Among the various barriers to moving a person who is on a civil commitment into a less restrictive setting are: a lack of guardian or supported decision maker; a lack of and inability to qualify for benefits; and/or no willing or appropriate nursing home placement. People with forensic commitments face multiple barriers, particularly when it is unlikely further hospitalization will restore competency.
At the date of this writing, over 60 people experience a barrier to discharge from the hospital into a more appropriate, less restrictive level of care.
Many people have more than one barrier, with the most common overlapping barriers being ties to the legal system for competency restoration, lack of benefits, and the need for a guardian. People who no longer need inpatient level care, but are unable to discharge, create a situation of inefficient use of hospital capacity that could otherwise serve individuals from the waitlist. The Statement of Need section of this report addresses how the system might improve to overcome these barriers and support people receiving the right care at the right place at the right time.
State Efforts
In addition to hospital enhancements and redesign efforts, Texas is focusing on strategies to eliminate gaps in order to increase access to outpatient mental health care. Two such initiatives include the Statewide Behavioral Health Strategic Plan (SWBHSP) (SWBHSP update) and the All Texas Access. The Strategic Plan is a five-year plan to address gaps in the mental health system. The All Texas Access focuses on LMHAs/LBHAs that serve at least one county with a population <250,000, i.e. rural counties. Its goal is to create regional plans to reduce the costs on local and state government while improving service delivery. The recent All Texas Access overview report, established the following legislature recommendations:
Consider amending Texas Health and Safety Code§573.012(h) to streamline emergency detentions,
Consider reducing grant match percentage for rural areas to allow greater participation,
Enhance collaboration among community mental health partners,
Consider building on the Broadband Development Council,
Evaluate innovations around telehealth in behavioral health services,
Increase support and training for mental health professionals,
Incentivize mental health deputy program and LMHA/LBHA collaboration, and
Continue to assess inpatient capacity for civil commitments.
Combined, the Strategic Plan, the All Texas Access, ASH Redesign and other state hospital projects collaboratively and with legislative support, can improve mental health care for Texans.
Pandemic Impact
While writing this report during a pandemic, it would be remiss to not mention how COVID-19 has impacted the current state of brain and mental health care and the capacity of the care continuum. Prior to the pandemic, research showed that one in five adults experience mental illness each year (Substance Abuse and Mental Health Services Administration, 2018). These rates are increasing with the lengthening pandemic. Texans are experiencing isolation, different daily patterns, job loss, stress from concern of contracting the virus, and stress of the economic downturn. Kaiser Family Foundation reported people struggling with mental health increased from 32% in March 2020 to 53% in July 2020 (2020). Meadows Mental Health Policy Institute projects that for every five percentages the unemployment rate increases in Texas throughout a year, an additional 725 Texans die from suicide and drug overdose (2020). The ongoing impact of COVID-19 will likely be felt for many years, even after the spread is contained by vaccines and other interventions. The increased need in brain (mental) health care caused by COVID will place pressure on a system in the midst of a redesign to care for the current needs, emphasizing the continued support and collaboration throughout Texas. The recommendations in this report will continue to support the growing mental health needs of Texans regardless of the cause.
Prior to the pandemic, research showed that one in five adults experience mental illness each year.
With these considerations in mind, the remainder of this report focuses on priorities and recommendations to complete the new Austin State Hospital, increase the functional hospital bed capacity to optimize the use of the new hospital facility, and strengthen Peer engagement to expand the care continuum.
Key Points – Service Area & Admissions:
• The ASH service area covers 75 counties: 38 counties for adults,
adolescents, and children; 19 additional counties for adolescents and
children; 18 more counties for children only.
• The percentage of admissions for forensic needs is continually increasing resulting in a corresponding decreasing capacity available for civil admissions.
• The total numbers of annual admissions is declining due to increasing lengths of stay.
• At the time of this publication, an average of 95 people are waiting for a bed at ASH, from a total of 1,000 waiting for a bed statewide.
• There are more than 60 people typically waiting to discharge from ASH each month, but are unable to discharge for a variety of primarily administrative reasons.
