03. Austin State Hospital Service Area
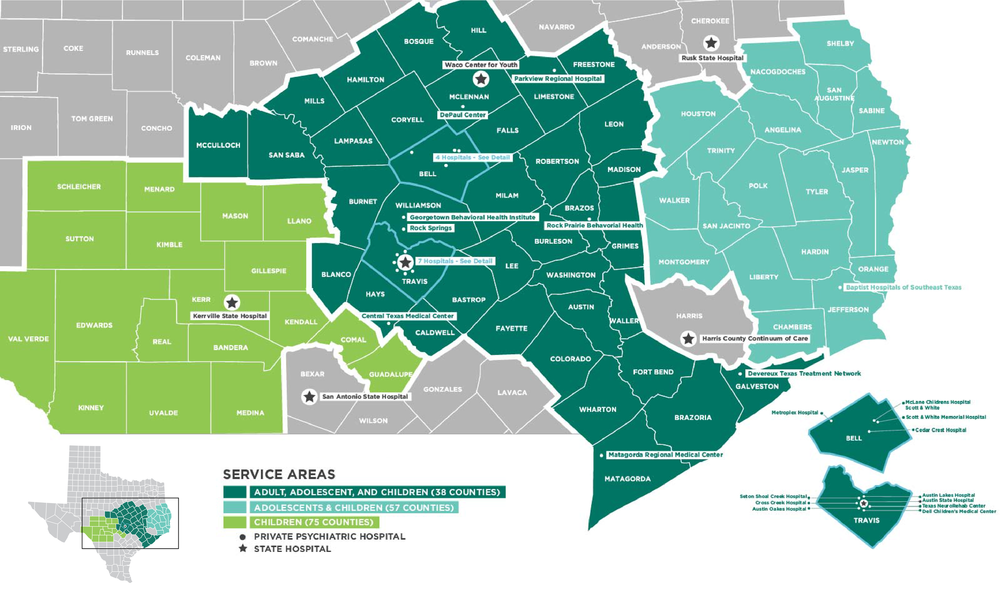
The Austin State Hospital service area includes 38 counties for adults, 57 for adolescents, and 75 for children. There are more than twenty private psychiatric hospitals in communities across the service area.
The Austin State
Hospital Service Area
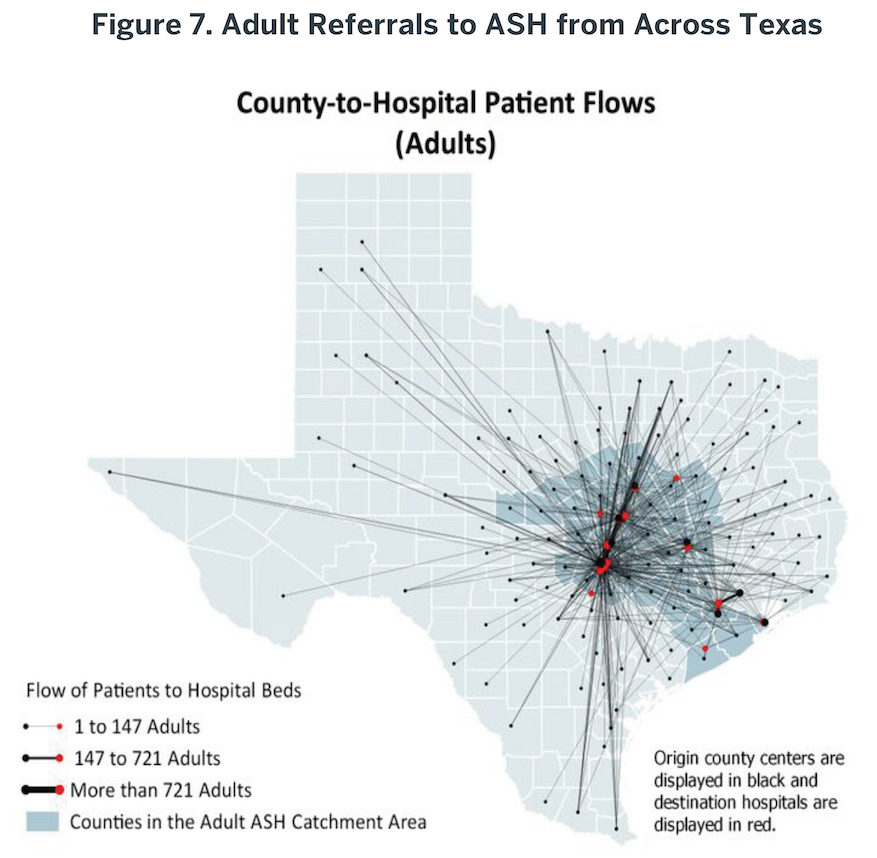
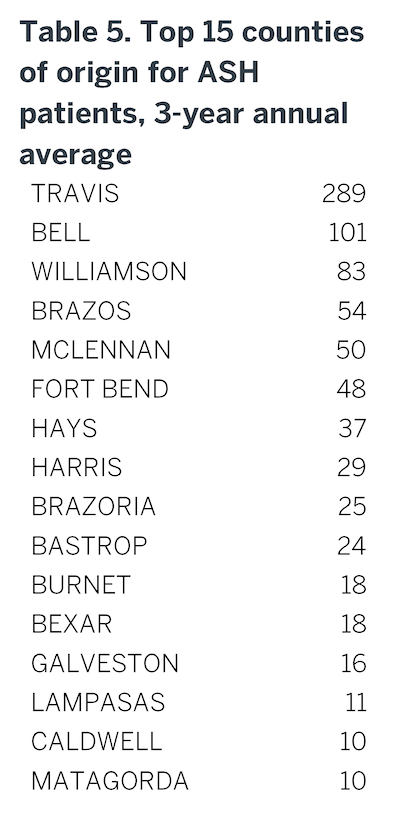
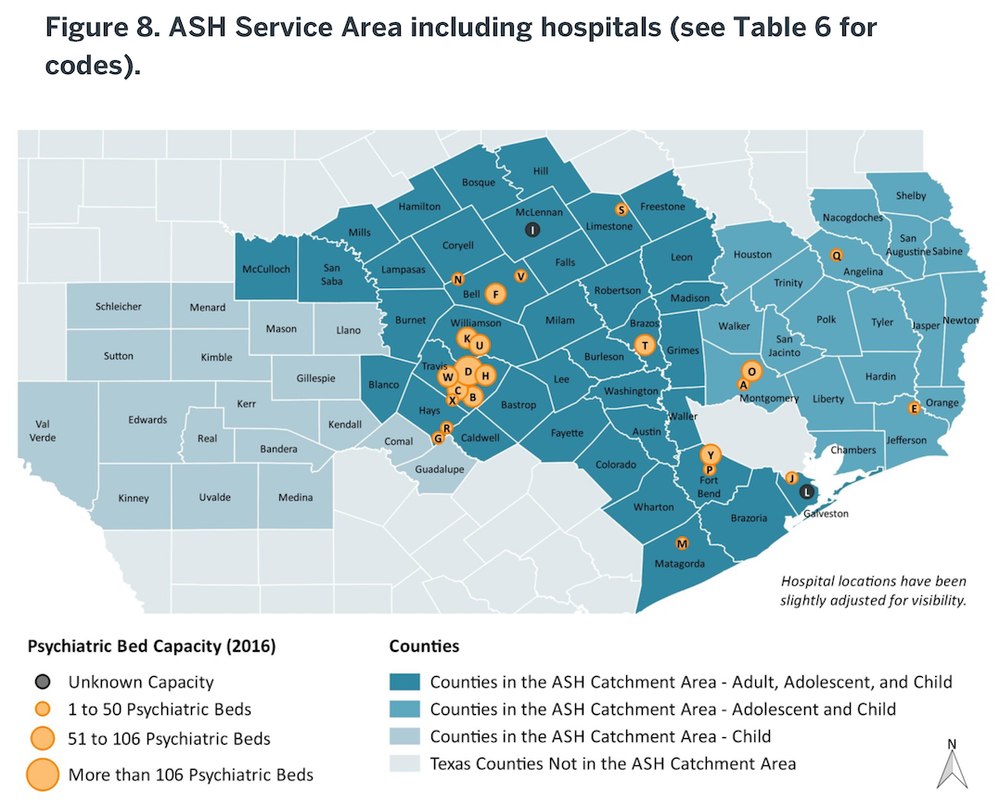
Although ASH receives referrals from throughout the state (Figure 7), it primarily serves a defined catchment area (Figure 8). Fifteen counties typically provide over 70% of the total number of referrals to ASH at any given point in time (Table 5), including counties that contain state-supported inpatient facilities (Bexar, Harris). Additional details are provided in Appendix 12.
As noted previously, waitlists for admission to ASH have developed for individuals requiring both forensic (criminal courts, jails) and civil (probate courts, other hospitals) care. In the ASH service area, approximately 95 people are on waitlists each day. Although people needing ASH admission can occupy emergency rooms or other healthcare facilities, most of these individuals (n=75) are ‘forensic’; consequently, they are waiting for transfer from a jail in which they may be receiving minimal psychiatric care. In particular, rural jails have significant problems identifying psychiatric support. These delays, then, extend people’s illnesses, contributing to poor clinical outcomes, in addition to increasing local (jails) and state (hospitals) taxpayer costs (Albert et al., 2017; Melle et al., 2008).
Fifteen counties typically provide over 70% of the total number of referrals to ASH…
In the ASH Service Area, about 2/3 of these individuals are waitlisted within Travis County with the rest scattered among the remaining counties (typically less than 6 individuals at any other site). County level distributions of forensic and non-forensic waitlists can be reviewed in Appendix 12. In the “Statement of Need and Recommendations” section of this report, we address potential solutions to eliminate these waitlists.
Inpatient Facility Utilization
In addition to ASH, there are several private psychiatric inpatient facilities distributed throughout the service area (Figure 8). Currently there are nearly 1,000 beds distributed among more than 20 facilities (see Appendix 12). They admit and treat more than 12,000 individuals annually. In contrast to ASH, which is always at full capacity, these facilities are usually less than 70% full. With consideration of a typical maximum capacity of 85% (the industry standard for short-term units), there are approximately 150 short-term acute care psychiatric beds available every day in the ASH Service Area. Inpatient psychiatric bed use in 2015 resulted in over $219 million in patient charges at ASH-area community hospitals. We estimate that hospitals received less than $87 million in payments for these charges (39%). Some payers, such as Medicaid, provide low reimbursement rates. In other cases, individuals treated did not have insurance coverage or income to cover hospital fees, so become hospital “write-offs.” These charges and payments are available by payer type in Appendix 12. Unfortunately, these low reimbursement rates disincentivize health systems from participating in psychiatric care, contributing in part to the shortage of access to brain health treatment.
Click to enlarge:
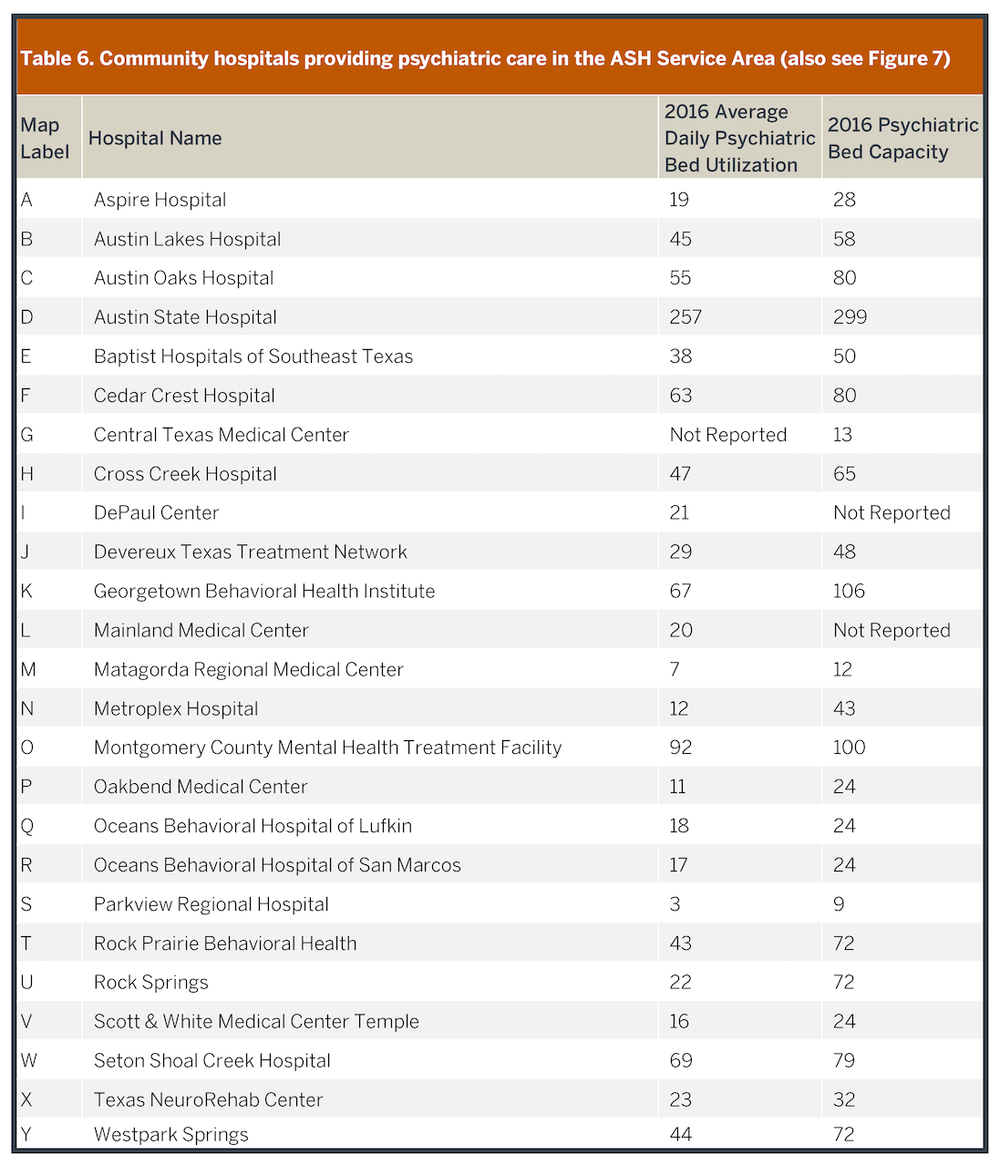
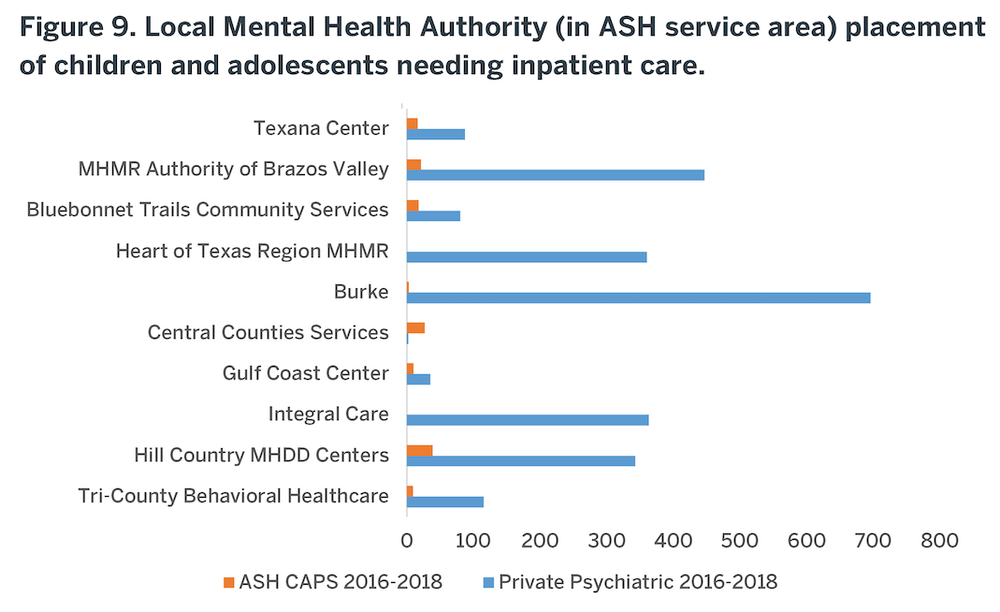
Many of these community facilities already work with Local Mental Health Authorities to sell beds for public patients as an alternative to ASH for short-term acute stabilization. Specifically, in FY17, nearly $17M was spent for Community Psychiatric Beds (CPBs) for uninsured patients who were treated within private facilities, paid for through LMHAs. The majority of child and adolescent psychiatric inpatient care throughout the service area – with both public and private payers – is provided by private hospitals (Figure 9) through these sources of funding which include: Community Psychiatric Bed funding, Psychiatric Emergency Service Center (PESC) funding, General Revenue Funding, and Medicaid 1115 Transformation Waiver Funding. Consequently, there are opportunities to expand the use of private hospital capacity to reduce waitlists in the jails and improve local access to care in the community. Although HHSC negotiated an average per diem payment for private hospitalizations statewide of $627, in FY17 that payment was $703 in the ASH Service Area and up to $1000/day in urban areas. Nonetheless, although some of these per diem costs to HHSC are higher than a bed day at ASH ($752), expanding access to private psychiatric beds using public funding ultimately provides better care by placing individuals needing short-term stabilization in a facility designed for that provision. Therefore, services are provided at a lower total cost of admission due to a significantly shorter length of stay, and usually closer to the person’s home. In other words, on balance, despite the higher unit (per diem) cost to HHSC, with the significantly shorter lengths of stay in private facilities and more rapid transition back into ambulatory care, it is less expensive to manage the episode of care in the community than in a state hospital. For example, a 10-day inpatient stay in a purchased bed in a community costs $7030 compared with $45,120 for 60 days in ASH. Using more purchased community beds also opens state beds for individuals whose illness cannot be stabilized in a short-term venue. This approach was recommended by the Cannon Report, as previously noted. Barriers to this approach (e.g. limited LMHAs funds for PPB) will need to be addressed to increase utilization of private hospital solutions, which are addressed later in this report.
Key Points – ASH Service Area: Inpatient facilities
• The Austin State Hospital (ASH) serves 38 counties for adults and 75 counties for children and adolescents, although 15 counties provide 70% of its admissions.• More than 20 private psychiatric facilities are also in the Service Area and typically have capacity available, up to 150 available beds daily.
• Private facilities are better designed for short-term acute stabilization so that, despite higher per diem costs, the overall admission is more effective, shorter and less expensive than one at ASH.
• Unused private psychiatric facility capacity offers an opportunity for improved and local access to care.
• Expanded mental health support to skilled nursing facilities provide a potential opportunity to eliminate the need for geriatric care within ASH.
Skilled Nursing Facility (SNF) Utilization
Of the 3.7 million adults living in the ASH Service Area, 549,308 people are 65 and older; although Texas is a relatively young state, this number is expected to grow by 38% by 2025. According to Meadows Mental Health Policy Institute prevalence data, 8,400 individuals aged 65+ have a serious mental illness. ASH currently is certified for 100 geriatric/specialty beds, although as noted, much of the Specialty Unit capacity has shifted to manage the increasing number of younger adults with legal charges. Consequently, in FY18, ASH’s geriatric annual daily census was 11 and there is no waitlist for services to this population. In part, this low use reflects the other, typically more appropriate, treatment opportunities outside the public system. In particular, skilled nursing facilities (SNFs) often provide long-term residential care for people with chronic conditions of severe and persistent mental illness, in addition to Alzheimer’s disease and other dementias. Specifically, there are 219 SNFs in the Service Area and most of them accept both Medicare and Medicaid. Together, these facilities provide approximately 24,000 beds. These facilities are best designed for managing typical conditions of aging, e.g., declining physical and cognitive health, although nonetheless manage severe and persistent mental illness as well. Their presence could provide an opportunity to embed mental health support through telehealth or other mechanisms to expand this capacity, thereby eliminating the need to care for older individuals within a state psychiatric hospital.
…most psychiatric patients can be managed for most of their illness course within outpatient settings…
Outpatient Service Utilization
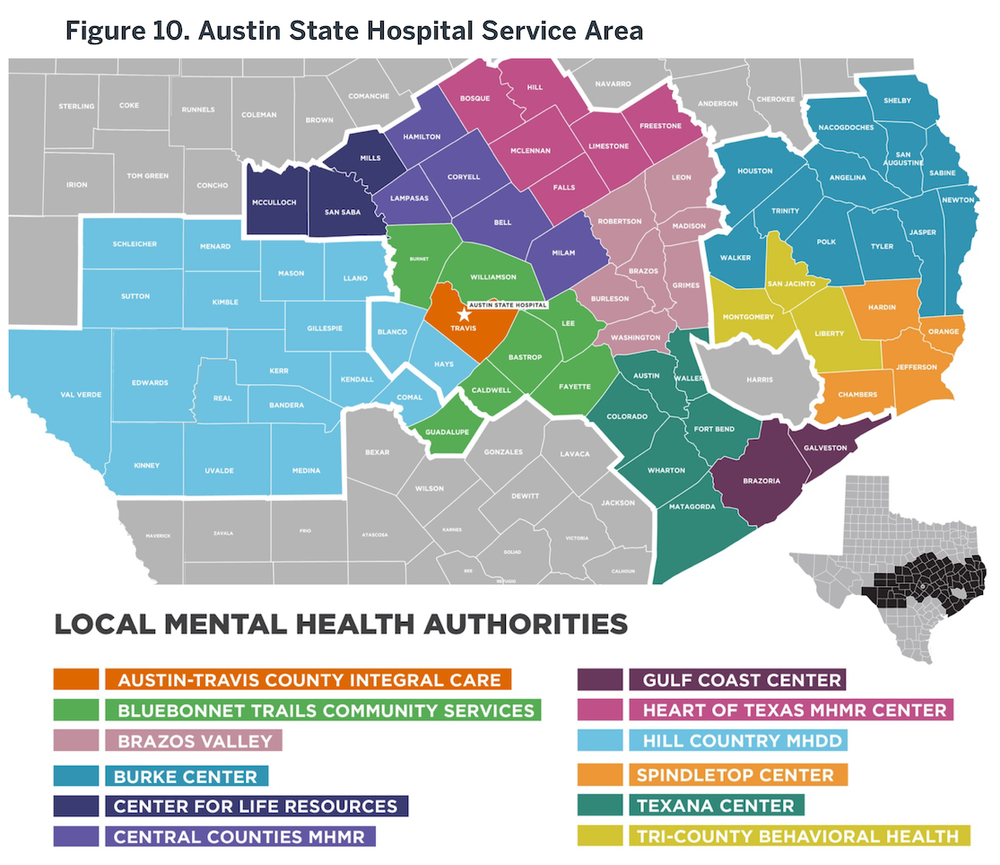
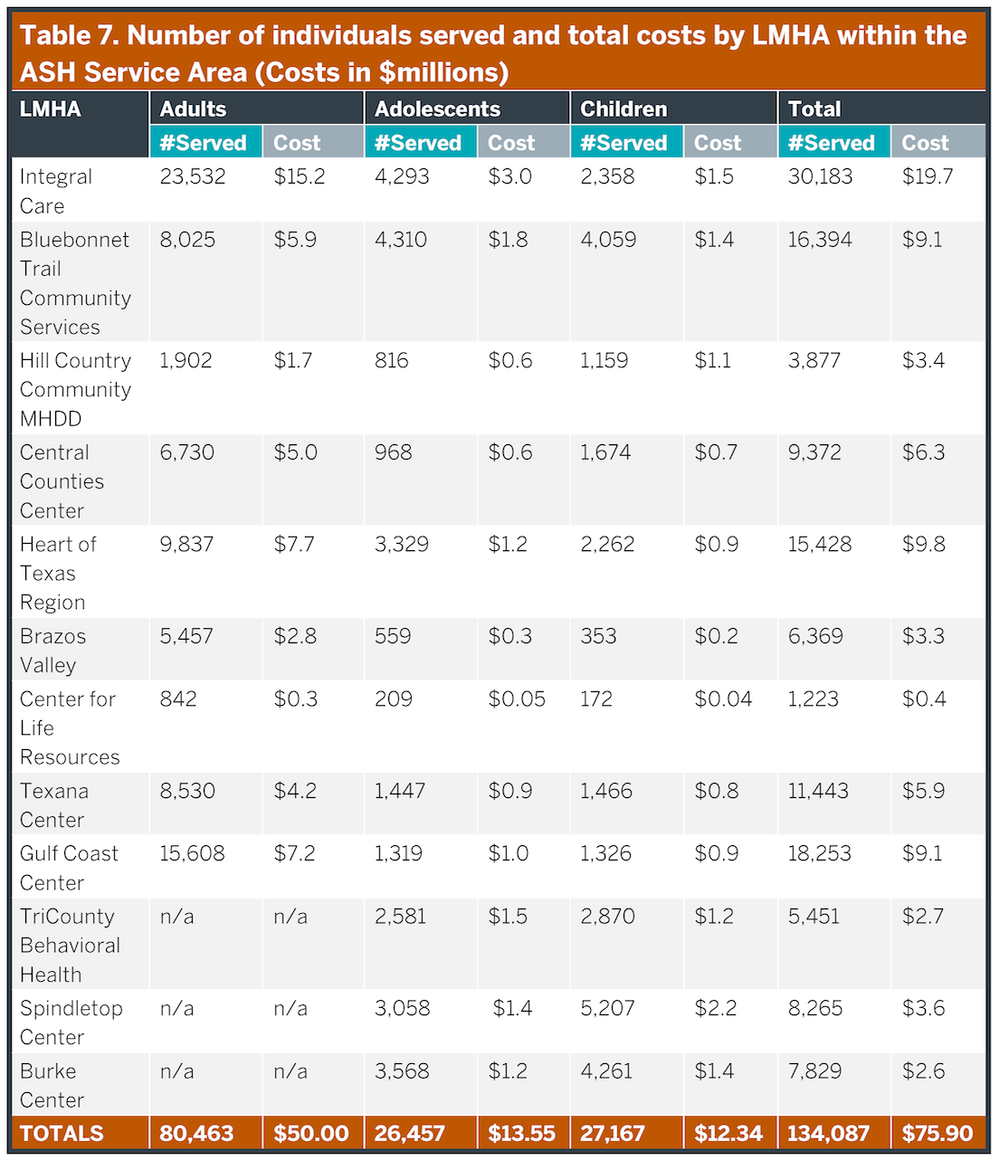
The function and performance of ASH depends heavily upon the care system within which it operates. As described earlier, ‘hospital capacity’ is heavily dependent upon how rapidly the beds ‘turn;’ optimizing bed turns depends on alternatives to hospitalization to provide care options (e.g., outpatient competency restoration) and on changes in both how people are admitted to and discharged from ASH. Most of the public mental healthcare within the ASH Service Area is provided, managed or funded by Local Mental Health Authorities operating within this region. Specifically, 12 LMHAs operate in full or in part within the ASH Service Area; the geographic distribution of these organizations are illustrated in Figure 10. Specific patient volumes and costs for these LMHAs within the ASH Service Area are listed in Table 7. Importantly, the LMHAs are operationally entirely separate from the state inpatient system, so that incentives between these two major components of public mental health care are not always aligned, as will be discussed later in this report.
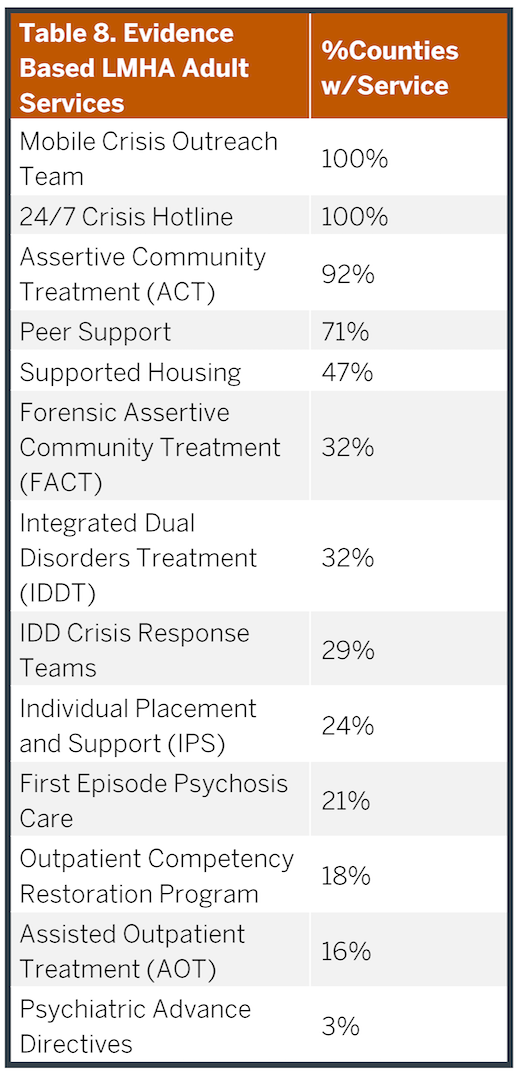
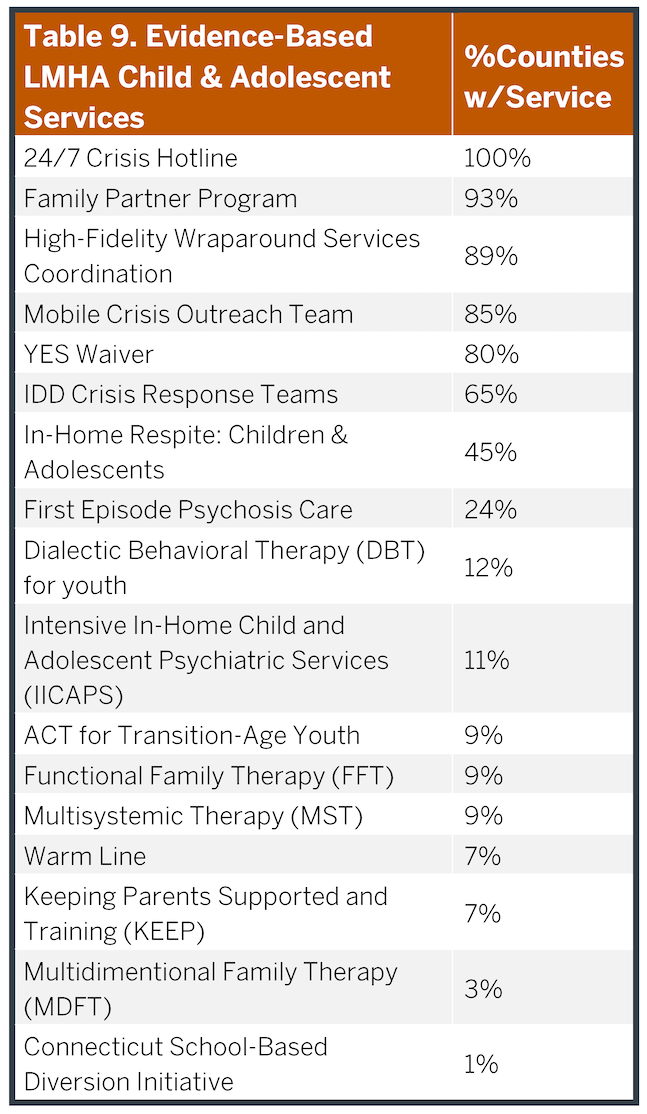
The LMHAs provide a broad array of services that are outlined in Tables 8 (adult) and Table 9 (children and adolescents). These services provide both acute and long-term outpatient care to manage brain health disorders across the region. In fact, most psychiatric patients can be managed for most of their illness course within outpatient settings as evidenced by the much greater number receiving these services each year (over 80,000) compared to those being hospitalized (1,000). These services vary across different LMHAs and counties creating care delivery gaps that are uneven across the state, particularly in less populated, rural counties. The bulk of patients served by LMHAs are individuals with severe and persistent mental illnesses such as schizophrenia, schizoaffective disorder, major depression and bipolar disorder. Although a number of other individuals also receive services based upon the severity of their disability and income; additional details regarding the service array, costs and people provided care within specific services are provided in Appendix 12. The types of patients served in the LMHAs and ASH are similar.
In addition to these direct care delivery services, the LMHAs play a critical role advancing school safety. HHSC has developed a school safety plan following events in Santa Fe (school safety). The safety plan builds upon Mental Health First Aid programs provided by the LMHAs. Since FY14 through FY18Q3, 25,318 school districts have been trained and 18,973 community members have been trained (MHFA_Report).
Click to enlarge:
LMHA Waitlist Data
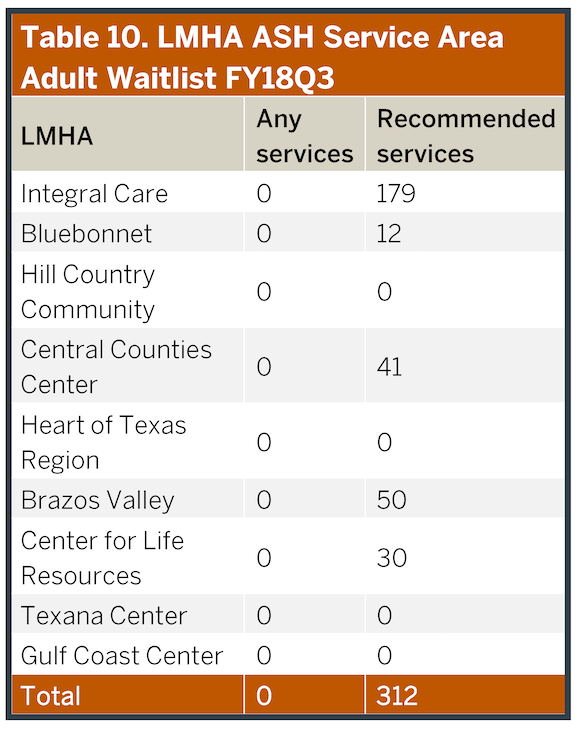
In FY18, LMHAs received extra funding from the state to support efforts to decrease their waitlists, and this effort has largely been successful. Of the nine LMHAs that provide adult services within the ASH Service Area, none currently have waitlists for general adult services. However, some individuals are receiving less than optimal clinical services due to staffing and funding limitations relative to specialized service demand (Table 10). Specifically, four of the LMHAs within the ASH Service Area have a waitlist for adults receiving care at a lower level than recommended. Among the 12 LMHAs serving children and adolescents, the waitlists for services is even lower than adults. No child or adolescent is waiting for services, although nine are receiving services below the recommended level (8 at Bluebonnet, 1 at Spindletop).
These data suggest that the LMHAs used the additional funding to close outpatient service gaps within the ASH Service Area. Discussions with the LMHAs within our work groups suggest that most are at or near capacity with current funding and staffing levels and some are struggling to provide specialized services as noted. These limitations disincentivize taking more discharges from ASH and reinforce the lack of integration between ASH and the ambulatory care system. Moreover, as noted in the previous section, as well as Tables 8 and 9, not all LMHAs provide the same breadth of services. Additionally, a number of limitations on the types of diagnoses and level of severity of individuals who receive services ensures a continued unmet need in these counties as discussed in Appendix 12 and the “Epidemiological Considerations” of this report. Consequently, in order to optimize the performances of (and investments in) new inpatient facilities throughout the state, including ASH, it will be critical to continue to advance ambulatory services delivered by the LMHAs.
Crisis and Emergency Service Utilization
Perhaps the most visible part of the mental health continuum occurs around crisis management, when major psychiatric conditions either first express or relapse into acute episodes of behavioral dysregulation. Crisis intervention is focused primarily on assessing individuals for safety to themselves and others and then providing disposition to additional care, that includes both inpatient and outpatient services. These services also provide short-term (typically less than 48 hours) stabilization in lieu of hospitalizations. Additionally, it is often within the context of an illness exacerbation and crisis that affected individuals intersect with the legal system, either because they have broken a law or because the police were called to help manage a crisis. Much, if not most, of this care is initially provided by general hospital emergency departments or within jails, although some counties also provide psychiatric urgent care, crisis stabilization or respite services independent of those venues. It is during crises that people struggling with mental illnesses are often most visible to the rest of society and hence crisis management is often the primary or entire focus of local mental health investment and service development. However, crisis services are only part of a continuum of care. Moreover, crisis services are among the most expensive available and their use could often have been avoided if services to alleviate or prevent illness exacerbations were more readily accessible.
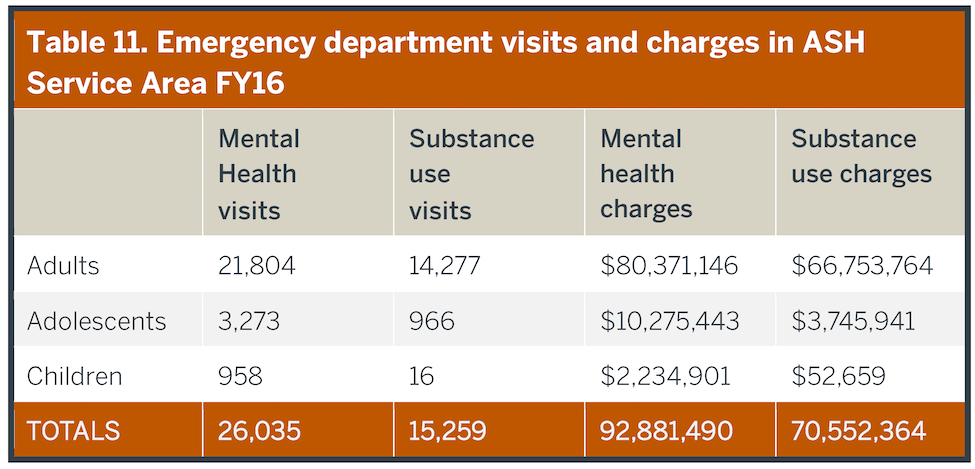
Within the ASH Service Area, more than 75 hospital emergency departments manage more than 26,000 visits annually that involve psychiatric disorders, and another 15,000 visits for substance use disorders (Table 11). This number includes more than 5,000 visits involving children and adolescents. Expenses related to these visits exceed $150M annually. From these visits, more than 7,000 adult, 2,000 adolescent, and 500 child psychiatric hospitalizations occur each year, with less than 3% of these directed to ASH, typically around 200 referrals per year with <20 being children or adolescents. Additional details are provided in Appendix 13. This rate of hospital admission from emergency visits (nearly 40%), is higher than expected from reports nationally, particularly for individuals without schizophrenia (NCHS Brief 215).
…there are inadequate next day or other transitional outpatient services, respite programs or crisis centers that would have been a better choice…
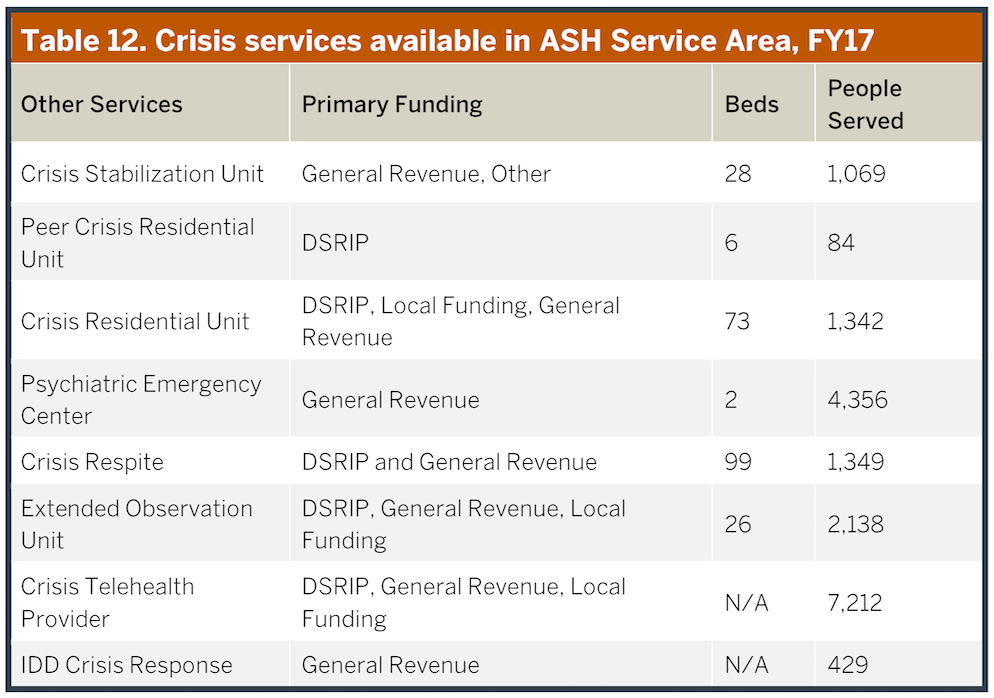
Often these admissions occur because there are inadequate next day or other transitional outpatient services, respite programs or crisis centers that would have been a better choice for disposition, both clinically and financially. These options are relatively limited in the Service Area, although have slowly begun to proliferate (see Table 12). Most jails and many emergency departments do not have easy access to psychiatric support leading to delays in care in the former and often excessive use of inpatient facilities for both. These limitations are particularly pronounced in rural counties, but even in urban areas the available psychiatric support can be limited (e.g., Travis county recently lost their only psychiatrist available to the local jail).
Key Points – ASH Service Area, Crisis and Emergency Service Utilization
• Over 75 hospitals provide 25,000 psychiatric emergency visits annually in the Service Area.• These visits account for nearly 10,000 hospital admissions per year, with about 200 going to ASH.
• The rate of hospitalizations out of emergency departments is higher than expected, likely reflecting the lack of alternative treatment options, particularly in rural areas.
• Alternative crisis interventions outside jails and emergency departments are proliferating, but not yet adequate to meet demand.
